
Why an MRI Disc Bulge Doesn’t Always Mean “That’s the Pain Cause”

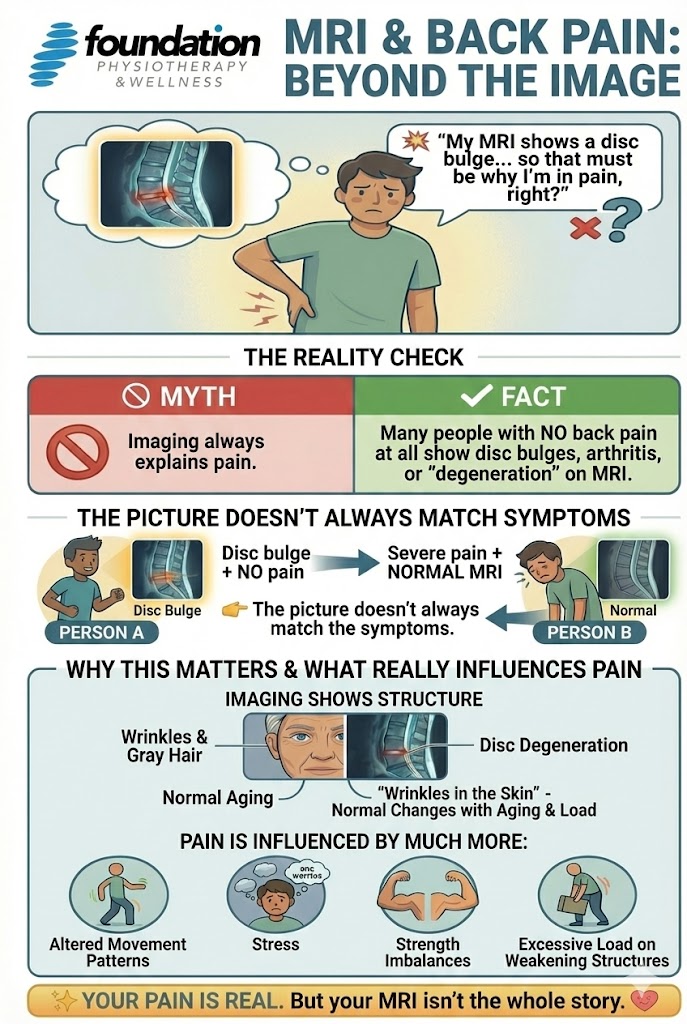
If you’ve ever had back pain and were told your MRI shows a “disc bulge,” you might naturally assume: “Well, that must be it — problem solved, right?”
Not so fast. Over the last decade, mounting evidence has shown that structural findings on MRI and the experience of pain don’t always match up.
In this post, we’ll dig into the research (including a 2015 meta-analysis) and explain what your MRI can tell you — and what it can’t. Then we’ll turn toward what matters more: movement, function, habits, and your unique context.
The Research Story: Lots of “Abnormal” Findings in Pain-Free People
1. The 2015 Meta-Analysis: High Prevalence of “Degeneration” Even in the Asymptomatic
A landmark 2015 systematic review and meta-analysis by Brinjikji et al. compared MRI findings in adults (50 years and under) with and without low back pain. PubMed+2PMC+2
Key findings:
- Among imaging features more prevalent in symptomatic individuals were disc bulge (OR ~7.54), disc extrusion, protrusion, disc degeneration, and Modic type 1 changes. PubMed+1
- But—and this is the critical nuance—many of these same findings were also common in asymptomatic people. In other words, a disc bulge or degenerative change doesn’t always come with pain. PMC+1
- Other findings (e.g. annular fissures, spondylolisthesis) were not strongly associated with pain. ajnr.org+1
The authors concluded: “Imaging features of spine degeneration are common in symptomatic and asymptomatic individuals.” PMC+1
Another related review also emphasized that the predictive value of MRI signs is limited — many “abnormalities” are part of normal aging, adaptation, or incidental. ScienceDirect

More Recent Evidence: Weak or No Clinically Meaningful Link
In a 2022 large cohort study, researchers looked at how MRI findings related to low back pain both cross-sectionally and over 6 years of follow-up. Lippincott Journals
They found:
- MRI degenerative features were present in both people with and without back pain.
- Most MRI findings showed only very small associations with pain severity (on a 0–10 scale).
- Most importantly, these imaging features were not strong predictors of future pain. Lippincott Journals
- In other words: having degenerative changes on MRI doesn’t mean you will develop disabling back pain later on.
So, the picture is consistent: MRI findings can be associated with pain in some cases, but they typically explain only a small fraction of why someone is hurting — and many people hurt even when their MRI looks “clean,” or vice versa.
Why the Mismatch? What Imaging Can’t Reveal
To understand why MRI findings and pain don’t always align, it helps to think about what an MRI actually measures — and what it doesn’t measure:
What an MRI Can Show
- Structural changes: disc bulge, protrusion, degeneration, facet changes, stenosis, etc.
- Static snapshots in the position the MRI was taken in (most often, lying down)
- Broad “damage vs no damage” categories
- Certain red flag features (fractures, tumors, infection)
What an MRI CANNOT Show
- Nociceptive sensitization (where pain is coming from), inflammation at microscopic levels, chemical irritation, nerve sensitization
- How tissues behave under load (i.e. prolonged sitting, walking, bending, lifting or twisting)
- How the nervous system interprets signals, psychological factors, pain thresholds and fatigue
- Pain modulation, muscle imbalances, coordination, posture under load, daily habits
Because pain is a complex, multifactorial experience, structural findings are only one piece of the puzzle.
Some other key contributors:
- Movement & biomechanics — how you bend, lift, twist, carry loads, especially under fatigue
- Muscle strength, control & endurance — weakness or poor motor control can add stress
- Load & recovery balance — overuse, repeated microtrauma, poor rest
- Sleep, stress, mood & central sensitization — the brain’s perception and processing of pain matters
- Past injuries, compensations & adaptions — your body carries a history
- Psychosocial and lifestyle context — fear, beliefs, habits, ergonomics, activity levels
Because of all this, many clinicians now talk about “non-specific low back pain”, meaning we can’t confidently say which specific structure is the pain source. The guideline approach is to treat the person, not just the MRI.
So, What Should You Do (or Think) If Your MRI Shows a Disc Bulge?
If you or someone you care for has MRI evidence of a disc bulge and back pain, here’s a more helpful mindset:
- Don’t panic — a bulge doesn’t imply danger, irreversible damage, or inevitable surgery. There are lots of people walking around with ‘disc bulges’, and do not feel a thing!
- Avoid over-attribution — just because it’s on there doesn’t mean it caused your pain. There’s a good chance the imaging results have been there prior to you experiencing pain.
- Focus on function — movement patterns, strength, stability, daily habits, load management.
- Use imaging wisely — rather than chasing findings, use MRI to rule out red flags or guide care when surgery is under consideration.
- Get a good assessment — work with a well trained physiotherapist or chiropractor to determine the root causes of your symptoms. Ensure they assess how you move, understand your history, aggravating/relieving factors, measure strength/flexibility, and identify contributing factors.
- Work toward input-based change — you can often reduce symptoms and improve function even if the “bulge” remains.
At Foundation Physiotherapy, our team is highly trained to help you through the process. We blend the imaging result with a full, individualized assessment. We look at movement, alignment, muscle function, load tolerance, posture, and your daily life — then build a plan to help you move better, stronger, more confidently.
Written by:
